There are several ways you can become deficient in GH, commonest one is after removal of pituitary tumour. Problem surrounding Pituitary gland, after radiotherapy, head injury, brain infection like meningitis, encephalitis you may become GH deficient. Although rare, Pituitary gland can become underactive in adults for no apparent reason called Primary Empty Sella Syndrome. How […]
Introduction to Pituitary
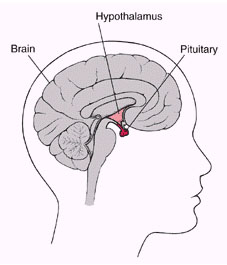
The pituitary is the master Gland controlling all the hormone-producing glands in our body. It is situated below the brain inside the skull bone.
Diagnosis of Pituitary gland problems requires experience and training in the field, maybe the reason why diagnosis and treatment of Pituitary gland issues are delayed.
In this section, we discuss the common Pituitary problems, their presentation and solution.
Diabetes Insipidus (DI)
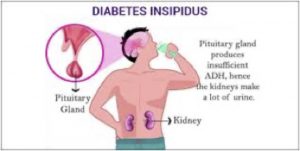
What is Diabetes Insipidus (DI)? diabainein: Greek, “to pass through” insipidus: Latin, “having no flavor” DI is defined as excess passage of large volumes (> 3 L/day) of dilute urine. What are the causes of excess urination (increased urine volume)? Diabetes Mellitus or sugar Diabetes, DI – due to deficiency of circulating Anti- Diuretic hormone- […]
Everything you wanted to know about Hypogonadism
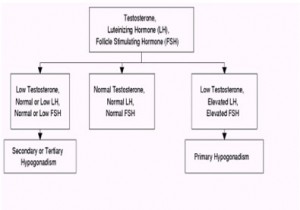
Normally two Pituitary hormones known as LH and FSH are responsible for stimulating Testes and Ovaries in men and women respectively. Any cause of hypopituitarism can cause hypogonadism. Hypogonadism can decrease other hormones secreted by the gonads including progesterone, DHEA, anti-Müllerian hormone, activin, and inhibin. Sperm development (spermatogenesis) and release of the egg from the […]
Everything you wanted to know about Acromegaly
Clinical Features The word Acro stands for peripheral parts and megaly means enlarged. Peripheral parts get enlarged giving rise to this facial appearance. Same happens with hands and feet. Treatment of Acromegaly Surgery of the Pituitary tumour is the treatment of choice, some cases do respond partially with Bromocriptine. There is a medicine available last […]
Pituitary Tumour Surgery

Once diagnosed with Pituitary tumour, we need to find out the extent of the tumour and most importantly the functional state of the Pituitary hormones. Prolactin secreting tumours can be managed by medical therapy. In a significant number of times Pituitary gland does not secrete hormone, so they cause pressure effect on surrounding structures or […]
Everything you wanted to know about Prolactinoma
Prolactin is a hormone secreted by the anterior pituitary gland which mainly plays a significant role in helping milk secretion in the postpartum period. What causes prolactin levels to go high? Drugs like Metoclopromide, Chlorpromazine, anti-depressants like Amitriptyline & Fluoxitene Underactive thyroid gland Prolactinomas – Prolactin-producing tumour of the pituitary gland. Prolactinomas occur most commonly […]
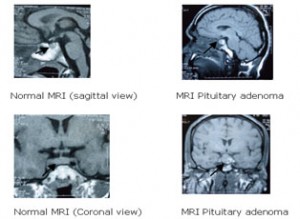
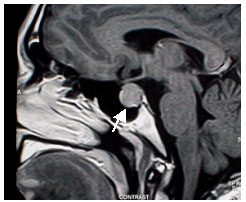
Pituitary: How to I know my Gland is ok?
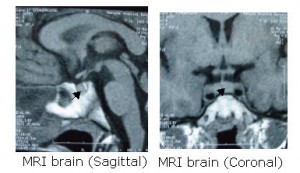
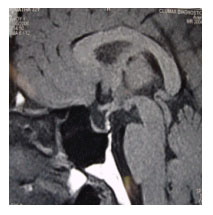
What hormones can be checked? All the hormones secreted by the pituitary gland can be checked using simple blood tests. How can I see the Pituitary Gland? The pituitary gland is best visualized by a MR scan of the brain, though an X-ray or a CT scan can throw some light on the anatomy of […]
Everything you wanted to know about Hypopituitarism
What is hypopituitarism? Hypopituitarism otherwise called as pituitary insufficiency refers to the low levels of circulating pituitary hormones. The clinical features of hypopituitarism are those of pituitary hormonal deficiencies. What causes hypopituitarism? Pituitary tumors Radiotherapy (pituitary, brain, nasopharyngeal) Inflammation of the Pituitary called Hypophysitis Invasion of the pituitary gland (Sarcoidosis, haemochromatosis) Empty sella syndrome (Pituitary […]
All you want to know about master Gland – Pituitary
Pituitary Gland has got two lobes: Anterior lobe and Posterior lobe What is its’ function? Each lobe of the pituitary gland secretes hormones, which in turn control the other endocrine glands in the human body Features of Hormone Deficiency or Excess
Pituitary Radiotherapy
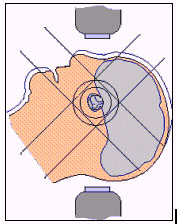
When is radiotherapy used? Reduce the size of pituitary tumors Prevent further growth of pituitary tumours Post-operatively to markedly decrease the chance of symptomatic tumour recurrence Reduce excessive hormone secretion (such as growth hormone or ACTH). How is radiotherapy given? A clear plastic mask made specially for each patient’s head, holds the patient’s head still […]