
What is Obesity? Obesity is too much weight for the height so that one’s health is affected. Body mass index best defines obesity. A person’s height and weight determines his or her body mass index. The BMI equals a person’s weight in kilograms divided by height in meters squared (BMI = kg/m2) Because of excess […]
Introduction to Hormonal Disorders
Hormones are chemical substances produced by special glands in the body and taken to different parts of the body by blood for action, most of them are life-saving meaning without them we cannot survive.
Some examples are Insulin, Thyroid hormone, Hydrocortisone. Others are very much needed for well-being for our day to day life. Hormonal problems are common and can be there at any age.
Like, growth hormone problem can affect the height of children, it needs to be treated in childhood only. Here in this section, we discuss common hormonal disorders and their solution.
What do I do with my Brittle Bone?
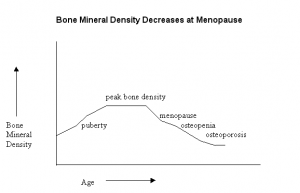
Osteoporosis is a disease in which bones become fragile and more likely to break. If not prevented or if left untreated, osteoporosis can progress painlessly until a bone breaks. Osteoporosis per se is not the major illness, but it is the complications of the disease that are the major cause of concern. Which are the […]
How Vitamin D is important for our good health?
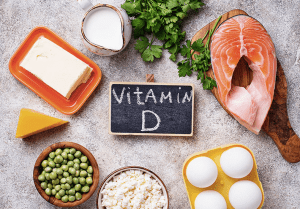
Vitamin D is a fat-soluble vitamin. The fact that it dissolves in fat is important, because it means the body can store it for future use. Ultraviolet B (UVB) in sunlight rays convert cholesterol in the skin into vitamin D. Darker skins need more sun to get the same amount of vitamin D as a […]
Is Osteoporosis same as Osteoarthritis?

What is Osteoporosis? Throughout the life, old bone is removed (resorption) and new bone is added (formation) to the skeleton. During childhood and teenage years, new bone is added faster than old bone is removed. As a result, bones become larger, heavier and denser. Bone formation continues at a pace faster than resorption until the […]
What is Osteomalacia?
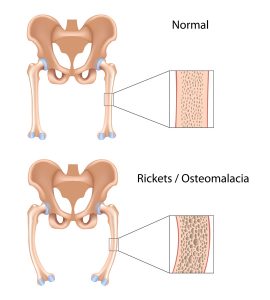
Osteomalacia is a defect in mineralization of bone. The defective mineralization is mainly caused by lack in vitamin D. Osteomalacia is derived from Greek: osteo refers to bone, and malacia means softness. What are the causes of Osteomalacia? Insufficient sunlight exposure, especially in dark-skinned subjects Insufficient nutritional quantities or faulty metabolism of vitamin D or […]
How do I keep my Calcium in the normal range?
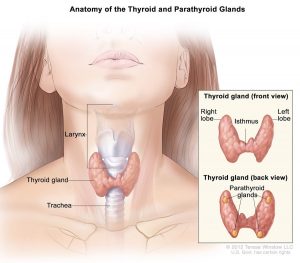
Calcium is important for the human as it helps in muscle contraction, nerve conduction, blood coagulation and release of enzymes & hormones. There are several regulatory mechanisms are there to keep blood calcium in the normal range, derangement of them can cause low or high Calcium in the blood. How is the blood Calcium regulated? […]
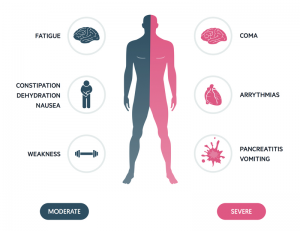
How can my Calcium go low?
Calcium is important for the human as it helps in muscle contraction, nerve conduction, blood coagulation and release of enzymes & hormones. There are several regulatory mechanisms are there to keep blood calcium in the normal range, derangement of them can cause low or high Calcium in the blood. What is Hypocalcaemia? Low level of […]
Why my blood Calcium has gone high?
Calcium is important for the human as it helps in muscle contraction, nerve conduction, blood coagulation and release of enzymes & hormones. There are several regulatory mechanisms are there to keep blood calcium in the normal range, derangement of them can cause low or high Calcium in the blood. What is hypercalcaemia? Hypercalcaemia refers to […]
How do I keep my Bones healthy?

Vitamin D allows your body to absorb calcium. Calcium is necessary for building strong and healthy bones. Without enough vitamin D and calcium, bones may not form properly in childhood and can lose mass, become weak. Good sources of calcium include dairy products (milk, cheese, yoghurt); calcium-fortified products (foods and beverages with added calcium), fish […]
How do I keep my kids Bone healthy?
Bones undergo changes throughout our lives, as old bone is broken down and new bone forms. But the most important time for building a strong skeleton is during childhood and adolescence. Bone strength depends on both the size of the bones and the amount of mineral they contain. The greatest gains in bone size and […]